When it comes to the adoption of simulation for training, perfection cannot be the goal. Optimization must be the goal. Do not wait, as this is the right time to adopt and get started on this path no matter what type of simulation technology is available for your discipline.
Even the most sophisticated flight simulators are only nearly perfect. The use of training devices in flight training started with the Link Trainer. The flight training devices evolved significantly over decades. Over this period, the flight training institutions or departments continued to derive value from these devices. It was based on prudent assessment and understanding of the capabilities as well as limitations and boundaries of simulation devices. Understanding the device is the first step to successful use. Procurement of devices is just a small step and marks the beginning of an interesting journey that often fails in the first few steps if not planned well.
I had introduced the term “Controlled Learning Experiences” in one of my presentations on simulation for training. In that presentation, distinct use of terms fidelity and realism had been suggested in order to ensure clarity in understanding and practice. The word “fidelity” must be used with training as in “Training fidelity”, while the word “realism” must be used with simulator devices as in “Simulator realism”. Click here for more details. The principal reason behind this is to focus on “Training Fidelity” as the products on market continue to evolve.
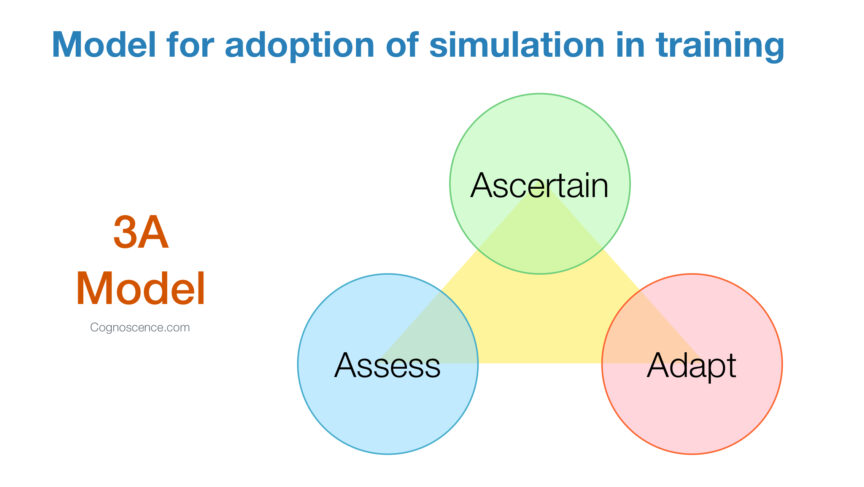
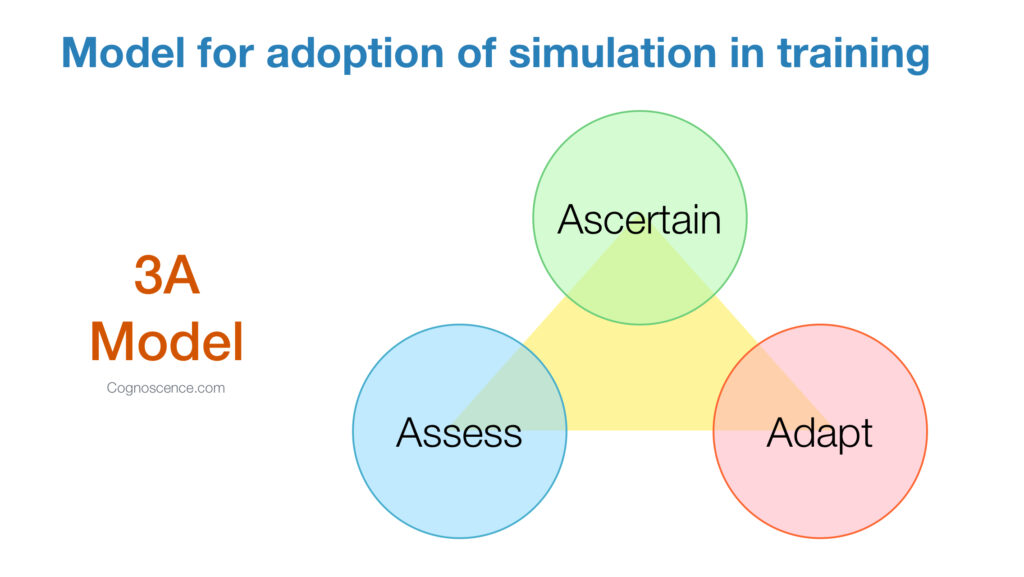
Consider this model for adoption of simulation in training.
- Ascertain the training fidelity that a well defined, structured use any simulator can be expected to deliver.
- Adapt the program to systematically integrate simulation training activities. This should be based a wide range of factors that vary across training institutions and programs. Ensure that all the necessary performance objectives are covered in the program. Providing access to simulator and assigning simulator training time is not sufficient to be considered training. This is even as simulators typically contain certain learning modules wherein self-directed learning can be undertaken.
- Assess using a reliable and valid tool. Assessment in various forms throughout the program delivery is essential for competency based learning and assurance of positive outcomes. Continuous assessment combined with feedback, support and remedial actions is a critical feature.
For those involved in any form of surgical simulation, it should be known that most training devices lack sufficient validation of the training outcomes. Further, the training outcomes vary significantly across studies. Rather, significant variation in training outcomes is a norm. With a significant investment and the potential benefits expected, it is important to invest in properly planning the adoption of advanced simulation. The use of the 3A model iteratively is highly recommended to start with and then optimize the outcomes over time. With time and experience, every important aspect of the program evolves, including the instructors, the simulation device, the courseware resources, and other complementary learning activities.
Go after Training Fidelity and not just after Simulator Realism.
Lead the way and do not wait for perfection. Do not expect it to be made easy for you. Only you can make it easy with a sound approach. Use the 3A model to discover what is best for your institution and be prepared to refine it as progress is made.